
Blog Post
Ethical AI in Healthcare: Balancing Innovation & Compliance
Learn how Claimocity uses ethical AI in healthcare with HIPAA compliance, coding rationale, and improved accuracy to protect patient data.
Is your practice throwing money away? Most providers would say “absolutely not.” However, studies have shown that healthcare practices typically lose 3–5% of potential revenue to compliance with current procedural terminology (CPT) coding and billing errors. BlueBriX Health estimates that poor billing and coding practices cost providers approximately $125 billion annually, with hospitals accounting for about $68 billion of that figure.
Much of this comes back to the structured summary of services that’s used to translate clinical work into billable claims for claims processing. It’s known as the superbill. Inaccurate superbills often lead to underpayment, claims denials, and billing audits across inpatient hospital settings and skilled nursing facility environments. Coding changes since 2024 have made older billing cheat sheets unreliable and more likely to cause errors.
There’s a direct correlation between reimbursement and how billing is handled. Inpatient practices that invest more in specialized billing support often see fewer denials and stronger revenue per encounter, with some data showing 1.3 to 1.8 times higher returns compared to practices that use lower-cost approaches.
Understanding how CPT coding works today is critical. The goal is to capture every billable service while maintaining CPT standards and ensuring accurate billing. In this article, we’ll talk about how the rules have changed, where the common pitfalls are hiding, and how to code and bill properly without adding admin tasks.
Healthcare reimbursement claims are submitted using CPT codes. They translate complex medical procedures into a uniform format. The CPT codes are bundled with diagnosis codes (ICD-10) and HCPCS codes, then sent to the payer for reimbursement. The payer uses the codes to determine the payment amount to be sent to the provider and the amount that the patient owes. When the correct codes are submitted, the provider will be correctly reimbursed for services provided without leaving revenue on the table. Accurate claims result in fewer denials, faster reimbursement, and reduced audit exposure due to compliance violations.
Correct documentation should be easy, right? During a busy day with a mix of clinical and administrative duties, attention to CPT coding detail can be lost in the shuffle. Add to that the increased complexity of CPT codes and the amount of information required in superbills, and it’s easy to see how errors can occur. However, coding must accurately reflect the services provided during inpatient admission, and the documentation must support medical necessity and level of care.
The AMA changes CPT requirements annually in an attempt to keep pace with evolving medical technology, new clinical procedures, and regulatory compliance. These are the most recent changes:
Since the most recent changes, observation care and inpatient admission codes now fall under a unified structure. This eliminates separate reporting pathways and simplifies coding for treatment facility workflows, but it also requires clearer documentation of patient status and level of care within a single code family.
Change 1: The observation care E/M code groups (99217-99220 and 99224-99226) have been deleted.
Change 2: The hospital inpatient code groups (99221-99223 and 99231-99239 and 99252-99255) have been updated to include observation care services.
The Evaluation and Management level is determined by either the complexity of Medical Decision Making (MDM) or the total time spent on the service. The patient’s medical history and physical exam are still required for care, and they used to be factors when choosing which codes to use for billing. That has changed. History and physical examination no longer contribute to CPT code level selection. Factors that affect MDM include the complexity of the problem, the data that was reviewed and analyzed, and the risk of complications or management decisions.
The requirements for time-based billing have changed, as well. Total time must be clearly documented for the date of service. That time should reflect only qualifying activities, such as reviewing records, patient evaluation, and care coordination performed on the same day. Non-qualifying time, including separately billable procedures, should not be included. Time-based billing receives increased scrutiny due to its variability and higher risk of misuse.
Time-based E/M coding doesn’t work the same way as other time-based coding. With many medical services, the requirements allow you to round up to the next unit once you pass the halfway point of a given time interval. E/M coding is different. It requires you to meet or exceed the full time threshold for a code before you can bill that code.
For example, if a code starts at 55 minutes, you aren’t allowed to bill that code at 54 minutes. You must reach the full 55 minutes to bill that code.
It gets a little more complicated when you’re billing for prolonged services. Additional time is counted in full 15-minute increments only AFTER you’ve exceeded the highest base code in that category.
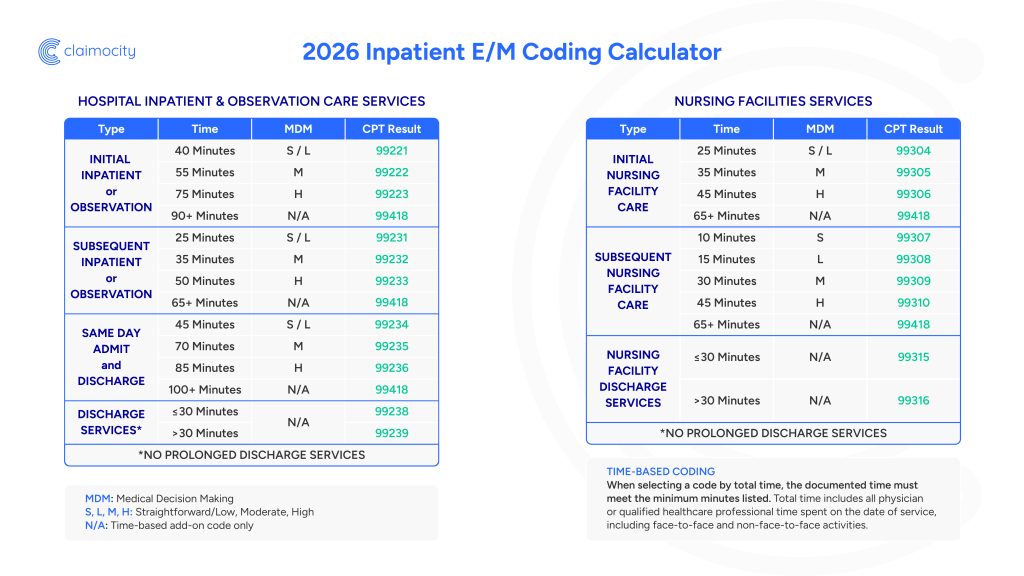
Here’s how time-based E/M coding looks in practice:
Initial inpatient services (time-based coding):
Prolonged time (add-on code 99418):
Subsequent inpatient services example:
The takeaway is pretty simple. Close doesn’t count. You must meet or exceed a code time threshold to bill for that code.
Coding inconsistencies, even those that seem minor, can have significant consequences on reimbursement and billing audits. Errors often result from misunderstanding updated CPT codes, documentation gaps, and misuse of time-based billing.
Upcoding occurs when a provider bills at a level higher than the supporting CPT codes. Payers use automated software, artificial intelligence (AI), data analytics, and targeted clinical audits to flag upcoding on claims. Downcoding is another problem. Providers will sometimes select lower-level CPT codes than supported due to uncertainty or conservative coding. This is a common mistake when MDM or time rules are misunderstood.
Both of these patterns create inconsistencies in billing data, which lead to increased payer scrutiny and denials. Downcoding results in lost revenue, usually in small increments that can become substantial losses over time. Upcoding is even more potentially hazardous, triggering repayment, penalties, and additional exposure to audits.
Superbills require a lot of information. It can be easy to leave them incomplete during the course of a busy day. Incomplete bills can be just as damaging as inaccurate ones. The most common errors are missing support for MDMs, lack of clarity around patient care decisions or complexity, and documentation that doesn’t align with billed CPT codes. As with inaccurate bills, these errors often result in failed claims validation during processing or payer review, which can lead to denials, delayed reimbursement, increased audit exposure, and in some cases, forced downcoding.
Time-based billing has its own set of issues that can lead to unsatisfactory results. The provider may not clearly document the time for which they are billing. They may also include non-qualifying activities or count time outside of the date of service. Using time when MDM actually determines the level can also create problems. Mistakes can make time-based billing inconsistent and more difficult to defend.
As a result, payers become more likely to audit and challenge reimbursements than they would have been with MDM-based billing. Time-based bills are at greater risk for audits, recoupments, and compliance issues.
All of these risks can be avoided without adding a mountain of admin tasks. The trick to accurate billing is to be sure your team has access to the latest CPT information and combine that with consistent documentation and internal validation processes.
One easy way to introduce errors into your coding is to use outdated billing cheat sheets. Guides created before 2024 rely on outdated information and don’t include changes that have been made to the CPT rules used in inpatient hospitals and skilled nursing facilities. There have been several key changes since 2023. History and physical exams are no longer used to determine the level of service, time requirements have been updated, and inpatient and observation services now follow a unified structure. Using guides that were created before these changes were made will result in coding errors and, ultimately, delays, denials, and audit exposure.
Whichever method you’re using to select the code, whether it’s MDM or total time-based, your documentation needs to clearly support it. For MDM-based coding, vague notes like “patient stable, continue meds” are no longer sufficient. Documentation must be more detailed, now. For example, documenting the complexity of the patient’s conditions, any data reviewed, and the level of risk involved in treatment decisions gives a much more accurate representation of the work performed.
The same principle applies for time-based billing. Where notes like “extended visit” may have been sufficient in the past, more thorough documentation is necessary, now. Include total time spent on the date of service along with the types of activities performed, such as patient evaluation, chart review, and care coordination.
With a more detailed account of the actual scope of care, you’re creating a clear connection between the services provided and the CPT code selected. That alignment pays off in the long run with fewer denials and improved billing accuracy.
Benchmarking gives your team a clear way to assess coding accuracy. It compares your coding patterns to peers in your specialty and helps to identify trends like overcoding or undercoding, as well as outliers in service or revenue code usage. These insights can highlight potential audit risks before payers do.
Review benchmarking reports regularly or use tools that automatically identify potential coding issues. Even small adjustments can significantly improve revenue, speed up reimbursement, and reduce compliance risk.
Get instant access to our inpatient E/M coding calculator and cheat sheets, built to make coding accurate, fast, and compliant:
Coding accuracy is extremely important for inpatient hospital and skilled nursing facility providers. It affects reimbursement, compliance, and long-term financial performance. The updated guidelines make it easier to code correctly, but only with detailed documentation and current workflows.
There are 3 things to pay close attention to so you can hit that sweet spot where you’re being paid for every service without compliance issues.
Working with a specialized inpatient billing or RCM partner can help you optimize your coding right away, rather than learning as you go. An experienced RCM team like Claimocity can lower your overhead, improve cash flow, and bypass the ongoing challenges of staffing and training. Studies have shown that outsourcing RCM lowers billing costs 30–40%. Outsourcing can also save time by eliminating in-house admin tasks, minimize errors and denials, simplify compliance and speed up reimbursements for greater revenue stability. Be sure to have the team perform a coding audit and an E/M coding review, and ask them to provide you with revenue projections.
Maintaining an inpatient healthcare practice grows more challenging every year. Margins shrink and compliance complexity grows. To grow your practice, you need to maximize your reimbursements, reduce your audit exposure, and maintain consistent billing accuracy across all health services.
We’re here to help. Request our free demo to find out what Claimocity can do to save your practice time and money.
Learn how Claimocity uses ethical AI in healthcare with HIPAA compliance, coding rationale, and improved accuracy to protect patient data.

Explore the risks of AI in healthcare and how Claimocity leads in safe, effective AI-powered workflows for inpatient providers.

Learn how to efficiently submit medical claims to enhance billing accuracy and expedite reimbursement with tips from Claimocity.