
Blog Post
Ethical AI in Healthcare: Balancing Innovation & Compliance
Learn how Claimocity uses ethical AI in healthcare with HIPAA compliance, coding rationale, and improved accuracy to protect patient data.
Every year, inpatient physicians brace for what CMS will do to reimbursement. This year came with a twist: the conversion factor actually went up. Why are so many hospitalists and SNF providers still looking at tighter margins?
On paper, 2026 looks stable. In practice, it may be one of the most consequential shifts facility-based groups have faced in years.
The conversion factor is only part of the formula. For inpatient providers, CMS’s restructuring of practice expense values may alter payment outcomes, positively affecting providers who see patients in LTC settings, while reducing reimbursement for many SNF-based visits.
This isn’t a dramatic across-the-board cut. It’s more subtle than that. The mechanics underneath the conversion factor have changed. Site-of-service differentials are widening. Small per-encounter shifts are being multiplied across thousands of visits.
In other words, a higher conversion factor does not automatically translate to higher payments. Site of service matters. RVU allocation matters. For many inpatient groups, the combined effect of these changes may result in flat or declining reimbursement in 2026.
If your 2026 projections assume that a higher conversion factor equals higher revenue, it’s time to take another look. The groups that catch the shift early will adjust. The ones that don’t may spend the first two quarters wondering why revenue isn’t lining up with volume.
In this article, we break down the 2026 Medicare Physician Fee Schedule (MPFS) Final Rule and explain what it means for inpatient providers, why it’s dangerous, and what they can do about it.
Medicare payments are calculated using two components: the conversion factor and relative value units (RVUs). CMS can adjust either one. That’s why a higher conversion factor doesn’t guarantee higher pay.
RVUs have three components: work, practice expense, and malpractice. For facility-based services, practice expense RVUs are already lower than non-facility care, because Medicare assumes the hospital or SNF absorbs most of the overhead. The 2026 rule reduced those facility-based practice expense RVUs further.
For inpatient providers, the conversion factor increase and the practice expense cut are pulling in opposite directions. Depending on your code mix and location, the cut can outweigh the raise.
The 2026 MPFS Final Rule includes several changes that affect inpatient providers differently than office-based physicians. While some updates appear positive at a high level, their combined effect can actually mean lost revenue for facility-based care.
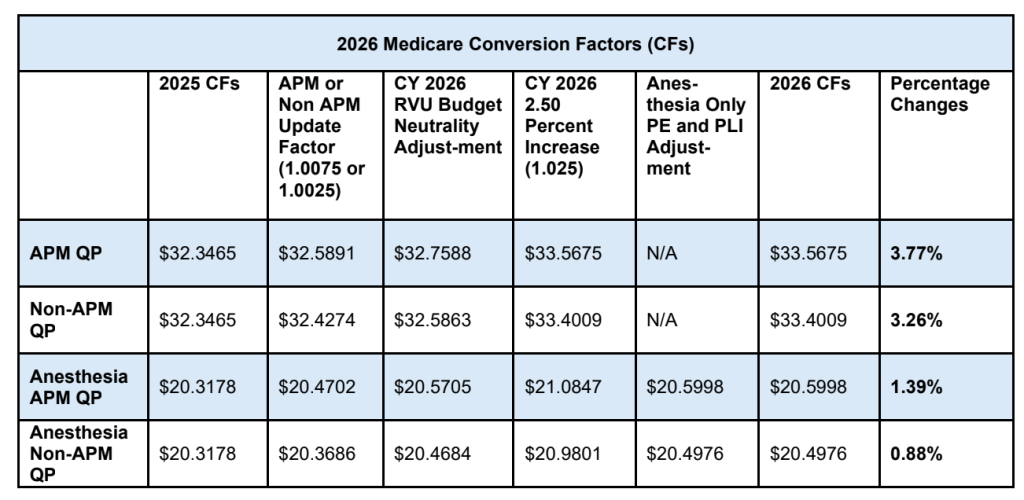
CMS finalized an increase to the Medicare conversion factor for 2026, including a 3.77% increase for Qualifying APM participants and a 3.26% increase for all other physicians. The increase reflects a temporary 2.5% pay bump, small updates to the baseline, and a positive 0.49% budget neutrality adjustment. On its own, a higher conversion factor would typically suggest higher reimbursement.
In LTC and SNF settings, the conversion factor increase does not operate in isolation. Other changes finalized in the rule directly affect how RVUs are calculated and allocated, particularly for services delivered in LTC and skilled nursing facilities.
As a result, the conversion factor increase does not apply evenly across all settings or services.
The part of CMS’s update for inpatient providers to pay close attention to is its practice expense methodology.
In facility settings, CMS assumes that hospitals and skilled nursing facilities absorb a greater share of overhead costs, such as staffing, space, and equipment. Under the updated methodology, CMS further reduced the practice expense RVUs assigned to many facility-based physician services.
This change shifts reimbursement away from physicians delivering care in facility settings and toward non-facility care, even when the clinical work and CPT codes remain the same. For inpatient providers, this redistribution can offset the benefit of the higher conversion factor and, in some cases, result in net decreases. You can see this shift most clearly in how Medicare treats certain place-of-service codes.
One example is the distinction between Place of Service 31 and Place of Service 32. POS 31 represents Skilled Nursing Facilities and is paid at the facility rate. POS 32 represents Nursing Facility or LTC settings and is now paid at the non-facility rate.
That means an encounter in an LTC setting may be reimbursed at a higher rate than the same CPT code performed in a SNF. The clinical work may look identical on paper. The clinical work and documentation may be identical. But the payment can differ based solely on the place of service designation.
For groups working across both environments, this isn’t a theoretical nuance. It directly affects revenue mix.
CMS also applied a broad efficiency adjustment as part of the 2026 Final Rule. Physicians who primarily provided services excluded from the adjustment, such as family medicine physicians and psychiatrists, will avoid the cut. However, CMS implemented a 2.5% cut to work RVUs, impacting most specialties by reducing overall payment by 1%.
While evaluation and management services are excluded from this specific adjustment, inpatient providers are not fully insulated from its effects.
Because many inpatient services are delivered exclusively in facility settings, they remain exposed to practice expense redistribution and budget neutrality dynamics that influence overall reimbursement. The exclusion of E/M services from the efficiency adjustment does not eliminate payment pressure for facility-based care.
CMS finalized several telehealth policies that directly affect inpatient and skilled nursing facility care, including:
While these changes preserve access to virtual care, they also increase the importance of accurate documentation, eligibility verification, and place of service reporting. As temporary pandemic-era flexibilities transition into permanent policy, CMS scrutiny around telehealth billing is expected to increase.
For inpatient providers, telehealth remains available, but compliance requirements are becoming less forgiving.
The financial impact of the 2026 MPFS Final Rule is not evenly distributed across specialties or care settings. Inpatient providers are more exposed than many outpatient physicians because of where and how their services are delivered.
Hospitalists, skilled nursing facility clinicians, and other inpatient providers deliver care almost exclusively in facility settings. Under Medicare’s payment framework, this means their services are subject to lower practice expense RVUs compared to non-facility care.
With CMS further adjusting practice expense methodology in 2026, facility-based physician services absorb a larger share of the redistribution. Providers who primarily bill in hospitals or SNFs have fewer opportunities to offset this impact through non-facility services.
In contrast, physicians who deliver care across mixed settings may see more neutral results, even within the same specialty.
When reimbursement pressure increases, operational accuracy becomes more important.
Place of service coding plays a direct role in how services are reimbursed. Errors between facility and non-facility designations can result in underpayment, overpayment, or increased audit exposure. In a year when margins are tighter, small inaccuracies can compound into meaningful revenue loss.
The distinction between POS 31 and POS 32 deserves special attention this year. POS 31 applies to Skilled Nursing Facilities and pays at the facility rate. POS 32 applies to Nursing Facility or LTC settings and pays at the non-facility rate.
Because POS 32 is reimbursed at the non-facility rate, it may result in higher payment for the same CPT code compared to POS 31. That difference is meaningful in 2026.
If documentation reflects an LTC environment but the claim is submitted under POS 31, revenue can quietly erode. On the other hand, inaccurately billing a SNF patient as POS 32 creates compliance exposure. The financial spread between these two codes makes precision more important than it has been in prior years.
CMS has signaled continued scrutiny around billing accuracy, particularly for services delivered in inpatient and skilled nursing facility environments.
Inpatient providers are also more exposed to documentation-related risk as CMS tightens enforcement across a few areas:
As reimbursement shifts and compliance standards harden, denied or downcoded claims carry a greater financial impact than in prior years.
For many inpatient providers, the disconnect between a higher conversion factor and actual reimbursement stems from this combination of factors: facility-based practice expense assumptions, site-of-service exposure, and operational sensitivity to billing accuracy.
This is why providers delivering care primarily in inpatient settings may experience decreased reimbursement revenue in 2026, even as broader Medicare payment headlines suggest increases.
To understand how these policy changes translate into real reimbursement impact, it helps to look at the codes inpatient providers use every day.
These are the foundations of hospital-based billing. Under the revised practice expense methodology, the conversion factor increase doesn’t apply evenly across all localities, so what looks like a raise on paper may not show up that way in your remittances.
High-volume for most hospitalist programs and entirely facility-based. Because these codes are billed repeatedly across a patient stay, even a modest per-encounter shift adds up quickly across a large group.
Accurate documentation and acuity capture matter more here than ever. Medicare already assumes significant facility overhead absorption for SNF services, and the 2026 methodology increases the weight of that assumption.
These codes often represent meaningful revenue in aggregate. Like the rest of your facility-based codes, the final payment depends on how the updated conversion factor and revised practice expense allocation balance out in your market.
Reimbursement varies by locality and MAC, so it’s worth running your highest-volume codes through your local fee schedule directly rather than relying on national averages.
Skilled nursing facility evaluation and management services, including CPT codes 99304–99316, follow the same pattern. These services are delivered in environments where Medicare assumes the facility absorbs a significant share of overhead.
Under the 2026 methodology, that assumption carries more weight. The resulting reimbursement change may feel disproportionate to the headline announcement of a higher conversion factor.
Discharge management services, such as CPT codes 99238-99239, along with inpatient critical care services (99291-99292), should also be reviewed carefully. These codes often represent meaningful revenue when aggregated across a large group.
As with other facility-based services, the final payment depends on the balance between the updated conversion factor and the revised practice expense allocation.
There is no single percentage change that applies across all inpatient services. The financial effect depends on code mix, site of service, and locality. For most inpatient groups, the safest approach is to review the specific CPT codes that drive the majority of volume and model the impact using their own regional fee schedule.
Start with the codes that represent the largest share of revenue. Model projected reimbursement using your local Medicare Administrative Contractor’s fee schedule rather than relying on national averages. Even small per-encounter shifts can compound across thousands of visits.
Evaluate how services are distributed across facility and non-facility settings. Groups delivering care almost entirely in inpatient facilities have limited ability to offset practice expense redistribution. Understanding your setting mix clarifies your exposure.
When margins tighten, leakage matters more. Review documentation standards for inpatient E/M, discharge, and critical care services. Confirm that place-of-service reporting aligns with actual care settings. Small coding inconsistencies can create avoidable revenue loss or audit risk.
Permanent telehealth flexibility does not eliminate billing risk. Revisit internal protocols around supervision requirements, originating site eligibility, and documentation of virtual presence. Clear standards reduce denial exposure.
Do not assume early 2026 remittances tell the full story. Track clean claim rates, denial trends, reimbursement per encounter, and days in accounts receivable over the first two quarters of the year. Variance analysis at the CPT level will surface pressure points faster than high-level revenue totals.
The practices that adjust quickly will have clearer visibility into the impact and more control over how they respond.
When reimbursement pressure increases, most inpatient groups feel it before they fully understand it.
It often starts with a simple disconnect. Volume looks steady. Clinical activity has not changed. Yet revenue trends slightly below projection. The difference is not dramatic, but it is persistent enough to raise concern.
In 2026, that gap is most likely to appear in high-volume E/M services delivered in facility settings. A small shift in reimbursement per encounter, multiplied across thousands of visits, becomes visible over time. Forecasts built on prior-year assumptions no longer align cleanly with actual remittances.
The impact also surfaces in workflow strain. Coding questions increase. Denials tied to documentation or the site of service require more review. Finance teams spend more time reconciling expected versus actual payment.
None of this signals failure. It signals sensitivity. When margins compress, variation carries more weight. A missed charge, an under-supported level of service, or an inaccurate site-of-service designation that might have been absorbed in prior years becomes measurable.
For inpatient groups, the response is not panic. It is precision. Reviewing code mix. Monitoring reimbursement trends at the CPT level. Confirming that documentation and billing are aligned. Creating visibility early, before small shifts accumulate.
Reimbursement headlines may suggest stability, but your day-to-day operations will tell the real story. In 2026, performance will depend less on policy language and more on staying ahead of gaps before they show up in financials.
By this point, most leadership teams are asking a more practical question: how exposed are we, and how can we react quickly?
What separates a manageable adjustment from a costly surprise is how quickly you can see what is changing. Do you know which five CPT codes drive the majority of your Medicare revenue? Do you know how those specific codes performed last quarter compared to this one? If reimbursement per encounter shifts, how long would it take you to catch it?
In a tighter reimbursement environment, those answers matter more than they used to.
Inpatient groups don’t need a complete overhaul to stay stable. They need clarity. Clean charge capture so encounters aren’t missed. Consistent documentation so levels of service hold up. Regular reconciliation between expected and actual payment so small variances get caught before they compound.
If your plan this year was built on last year’s Medicare rates, it’s worth revisiting your projections now. Start with the CPT codes that drive the bulk of your volume, run them through your local fee schedule, and compare expected reimbursement per encounter to actual remittances as the year gets underway.
Updated reimbursement projections ripple through your whole operation. When your revenue baseline is accurate, coverage decisions, payer contract discussions, and compensation planning all get sharper, too.
The groups that stay steady in 2026 will be the ones that measure early, reconcile often, and adjust projections based on what the data is showing in their market.
The 2026 rule is finalized and already in effect. For most inpatient groups, the impact won’t arrive as a single obvious event. It shows up in remittances that trend slightly below projection, denials that take a little longer to resolve, and monthly revenue totals that don’t quite match what the budget assumed. By the time the pattern is obvious, you’ve already lost ground.
Staying ahead of that means having visibility into your highest-volume codes before the gaps widen. It means clean charge capture so every encounter makes it into the revenue cycle, accurate documentation, so the level of service billed is the level that gets paid, and consistent reconciliation between what you expected and what actually came in.
That’s the work. It’s a lot to manage alongside everything else your team is responsible for.
Inpatient billing is all we do. Claimocity combines AI-powered charge capture with end-to-end RCM services, purpose-built for facility-based care. Our charge capture helps providers understand why a code is appropriate, not just what to bill, so documentation and coding stay aligned even as CMS tightens its methodology. Practice IQ gives your leadership team a centralized, real-time view of financial performance so you’re never waiting on a month-end report to know where things stand. And our dedicated US-based teams work alongside your group every step of the way.
Want to see what that looks like for your group? Let’s talk.
Learn how Claimocity uses ethical AI in healthcare with HIPAA compliance, coding rationale, and improved accuracy to protect patient data.

Explore the risks of AI in healthcare and how Claimocity leads in safe, effective AI-powered workflows for inpatient providers.

Learn how to efficiently submit medical claims to enhance billing accuracy and expedite reimbursement with tips from Claimocity.